























1. The Hazards of Postprandial Hyperglycemia
An elevated blood glucose level after meals does not simply mean a “temporary spike.” Research has shown:
- Independent risk factor: Postprandial hyperglycemia significantly increases the risk of cardiovascular and cerebrovascular events, even when fasting glucose and HbA1c are within the normal range (DECODE Study Group, Diabetologia, 1999).
- Doubled risk: In people with otherwise normal glucose profiles, isolated postprandial hyperglycemia can more than double the risk of cardiovascular mortality (Funagata Diabetes Study, Diabetes Care, 1999).
- More insidious damage: Compared with elevated fasting glucose, postprandial hyperglycemia causes greater vascular endothelial injury and accelerates atherosclerosis (Ceriello A., Diabetes Metab Res Rev, 2000).
Over time, poor control of postprandial glucose not only increases the risk of angina, myocardial infarction, and stroke, but also worsens diabetic complications such as retinopathy, nephropathy, and neuropathy. Controlling postprandial blood glucose is therefore an essential protective measure for cardiovascular health.

2. Postprandial Blood Glucose Targets for Different Populations
Postprandial hyperglycemia is generally defined as blood glucose >7.8 mmol/L (140 mg/dL) at 1–2 hours after eating. However, treatment targets differ among populations:
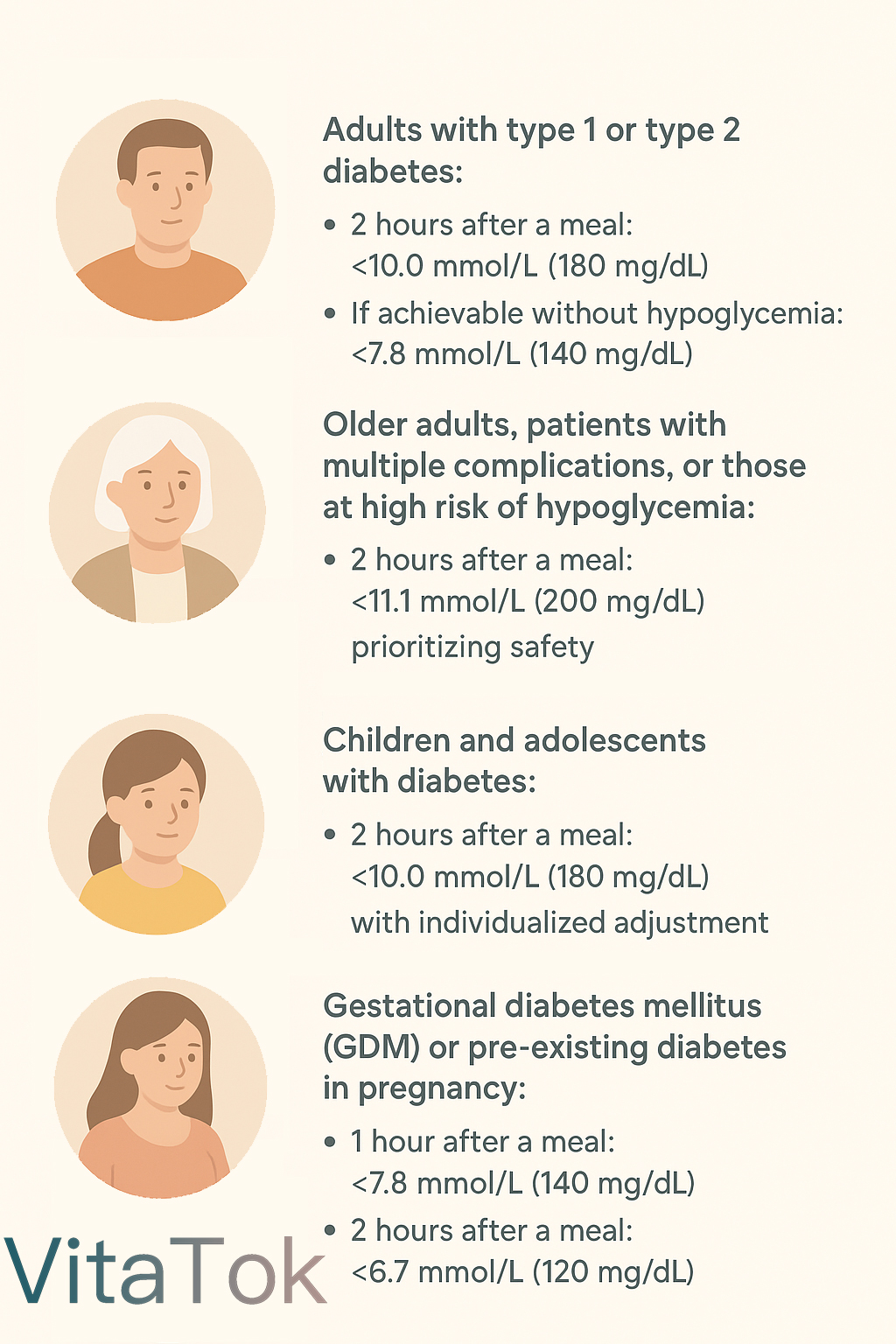
- Adults with type 1 or type 2 diabetes:
- 2 hours after a meal: <10.0 mmol/L (180 mg/dL, ADA guideline).
- If achievable without hypoglycemia: <7.8 mmol/L (140 mg/dL, AACE guideline).
- Older adults, patients with multiple complications, or those at high risk of hypoglycemia:
- 2 hours after a meal: <11.1 mmol/L (200 mg/dL), prioritizing safety.
- Children and adolescents with diabetes:
- 2 hours after a meal: <10.0 mmol/L (180 mg/dL), with individualized adjustment.
- Gestational diabetes mellitus (GDM) or pre-existing diabetes in pregnancy:
- 1 hour after a meal: <7.8 mmol/L (140 mg/dL).
- 2 hours after a meal: <6.7 mmol/L (120 mg/dL).
- Healthy individuals:
- 2 hours after a meal: <7.8 mmol/L (140 mg/dL).
In summary:
- Adults: <10 mmol/L at 2 hours; <7.8 mmol/L if aiming for tighter control.
- Pregnancy: strictest targets.
- Older adults: targets may be relaxed to prioritize safety.

3. How to Improve Postprandial Hyperglycemia
Managing postprandial glucose requires more than simply “avoiding sugar.” Comprehensive strategies include:
1. Medication optimization
- Adjust medications under medical supervision; in some cases, intensification of prandial insulin or oral agents may be necessary.
- Do not stop or change doses without physician guidance.
2. Dietary adjustments
- Control portion size of starchy foods such as rice, noodles, and bread, but avoid long-term very low-carbohydrate diets, as moderate carbohydrate intake is important for overall energy and metabolic health.
- Meal sequencing: eat vegetables and protein first, followed by carbohydrates, to slow glucose absorption.
- Choose low-glycemic index (GI) foods such as brown rice, whole wheat bread, oats, and legumes.
- Incorporate acidic foods (e.g., vinegar, lemon juice) to slow gastric emptying and attenuate glucose excursions.
3. Post-meal activity
- Engage in light to moderate exercise (e.g., walking, household chores, stretching) for 20 minutes, starting 15–30 minutes after a meal.
- Avoid lying down or remaining sedentary immediately after eating.
- Refrain from vigorous exercise right after meals, as it may cause glucose fluctuations or hypoglycemia, especially in those using insulin.
4. Lifestyle and monitoring
- Maintain regular sleep patterns; avoid staying up late.
- Manage body weight; minimize late-night snacks and sugary beverages.
- Use continuous glucose monitoring (CGM) to track postprandial glucose trends in real time, and adjust diet and exercise strategies accordingly.




